
Returning to running postpartum in Philadelphia
As we passed the Philadelphia marathon sign-up window, I was reminded of the training windows for races. Typically I have followed the 4 months out for Marathons (admittedly I've only done 1) about 2 months for ½ Marathons and about 6 weeks for Broad Street (10 miles). But looking at windows of time for training also gets me thinking of the 6 weeks postpartum when you essentially get “cleared” for everything and yet nothing. Your OB did not extensively study biomechanics and exercise science to determine when exercise activity should resume. In that same context, if you report that you don't have any pelvic floor (PF) type symptoms at that follow up or pain, you essentially are left to figure that out on your own. (And that will be another blog post at some point: Why every mom should have PT postpartum)
Fortunately for the vast majority of us existing in the last decade, searching for this information is plenty, and you do get an idea of what a ‘return to run’ or ‘return to the gym’ routine is, if you search for it. But what if you don't? Or what if there is actually just too much?
For the number of people that prep with all the pregnancy knowledge and birth prep, there are just as many people not doing that, and a far greater amount of people that lie somewhere in between. And honestly there is just time and bandwidth to think through all of this postpartum.
So this is for those people lingering in the middle of the super planning to I didn’t do anything: you did the search but overwhelmed with the info, but know more than just to wing it.
The Mindset:
A good way to approach returning to running is a bit of structure, and a bit more intuition of your body. If you are experiencing no pain or symptoms (think PF symptoms, heaviness) then you are listening to your body for a safe progression. And what that means is thinking about pressure, discomfort and even pain, as signals and warnings, not necessarily stopping indicators.
Listening to your body for a runner or athlete brain though is a different mindset postpartum then pre. This is your reminder that your body is no longer the one you were running with before creating life and carrying that life for the last 9 months. It's the reminder that your body is tired, you are recovering from a birth, not just a couple weeks of not training.
Someone returning to running with no symptoms leading up to your clearance, you are going to listen to your body for things such as pressure, pain, discomfort, difficulty breathing, general increased fatigue. Again, not indicating an automatic stop, but more of a consideration that the training load might have to be changed. It’s recognizing the system may not be ready for the demand yet.
You ran 1 mile, and felt heaviness starting at mile .5, or leaking .25 into it? Then modify it. Run 0.1-0.2 then walk 0.25-0.5. Build off of that.
Sometimes we like to keep people in these rigid programs, and while some people like the structure, it is also totally fine to wing it, with the understanding of what you might be experiencing. For the same amount of people that I have programmed some very thorough return to running programs, I have also had just as many clients tell me “I just went for it” and they were fine.
Other things to consider:
While walking/running can be an easy avenue to return to, there are some other things I like to remind my clients. No just endurance or running stamina was affected and these are also not the only systems that need to be looked at.
Biomechanics: Hips widened. Load was changed(hello to me gaining an extra 50lbs with my first pregnancy). Abdominal muscles were stretched. Muscles or hips, back and legs potentially were weakened due to changing structures or decreased activity.
Cardiovascular: Heart rate changes. Blood volume changes. Cardiac output changes. Fluid redistribution (ie reducing swelling in body)
Mental Health: Identity changes. Postpartum depression/anxiety. Sleep deprivation. Caregiver responsibility.
Calorie Demand: Recovering postpartum alone requires 300-500 of additional calories as compared to a pre-pregnancy need, and if you are breast feeding, those numbers are even higher.
And this is by no means an extensive list, nor a specific list to you. I have had clients over the years that had no ability to maintain a typical exercise routine during pregnancy due to severe morning sickness or Hyperemesis Gravidarum, so their concern for just being able to keep enough calories in their body to make it through a pregnancy was a bigger priority.
There is no perfect plan:
Research is very supportive of the benefits of being active during a pregnancy to improve outcomes postpartum. And we know of all the benefits of general exercise for humans and longevity and health, as well as those benefits of postpartum mothers. But this is also the reminder that if your return to running or gym is just not in your priority list now, thats ok. We don’t have anything yet that says whether you return at 6-12 weeks vs 6-12 months is any different in long term outcomes. But what we do know is returning to exercise should be a goal.
Too often we are falling into the extremes: our bodies can do anything and can push through anything, OR everything must be progressed steadily and slowly. I have known people in both camps and have been successful, but our bodies and their capabilities are so much more nuanced than that. We have sleep schedules we are working on, breastfeeding happening in the middle of the night, returning to an office setting, worrying about the sound of congestion.
And while I will always support exercise as a necessary part of our health, what the exercise is, does not nearly hold as much weight. I will always be supportive of what you are able to do, and do consistently over time. Activities that can be modified I will always direct people towards just because it's something that can still be done with different lenses. A return to running can be changed with walking intermixed, speed, distance, elevation etc. And if that modification can get someone back to a goal of theres sooner, I will always be in support of that.

Your Pelvic Floor Symptoms Might Not Be a Pelvic Floor Problem
When a new client presents into the clinic, a lot of times they have sought me out because of their pelvic floor symptoms. They explain a history of leaking and heaviness at times when doing higher level activities. They googled the symptoms and have decided their core and pelvic floor must be weak following their pregnancy, and they have tried adding kegels and core work into their routine, thinking that will help, but nothing changes.
Then they find me and I will ask them: “What if your pelvic floor isn't the problem, what if that is just where your symptoms are showing up?”
The look of question and shock usually is what is next on their face and then curiosity, wondering how their leaking cannot be a pelvic floor problem? And then begins the sometimes nuanced education of the pelvic floor in our bodies, and what messages it can be telling us.
Sometimes the isolation of pelvic floor therapy has separated how we think of the pelvic floor as a separate entity, rather than how it's working together as a part of a system.
What Is Pressure Management?
What is intra-abdominal pressure (IAP)? I often teach clients to look at our trunk as a canister. We have the diaphragm on top of the canister, on the bottom we have pelvic floor, and supporting the sides we have abdominals and spinal muscles. When we breathe, that canister has to adjust to the pressure. On the inhalation, our diaphragm lengthens, moving down into the abdominal cavity to allow the lungs to fill with air. Our pelvic floor also lengthens, accommodating that change, as well as our belly and back expand.
When we exhale, the opposite happens, diaphragm returns, as well as all the other aspects of the canister. What is moving between the top and bottom are all our guts: think intestines, liver, bladder etc. Specifically things like peristalsis (involuntary movement of the gastrointestinal (GI) system) requires this movement to actually be able move things throughout our GI system.
As the air is moving in and out of our bodies, the canister has to adjust. It has to manage that change in pressure to allow for the body to function well while allowing the air in and out. When things are being managed well we think of the pressure being distributed well throughout the whole canister aka abdominal cavity.
However, sometimes that pressure system can get disrupted. Meaning the pressure gets dumped into areas that are not meant to be managing the overload of pressure, or it's an area that may have had some weakness, but now is just not able to keep up, and that is where your body is showing symptoms. While I am specifically speaking right now on pelvic floor symptoms, this can be the same logic of back, pelvic, hip, and shoulder pain as well.
What Happens When Pressure Isn’t Managed Well
If pressure isn't getting to areas in that body well, sometimes that pressure ends up in a more downward direction on the pelvic floor. And then sometimes, those muscles, due to previous history, may not be as coordinated as they once were, or have a delay in activating when they are needed. And other times, our body (in its sometimes amazing wisdom but unhelpful solution) picks up different habits to help offer a different management strategy such as breath holding or bracing, that doesn't match the requirement long term, overloading the pelvic floor.
And what do people notice? They don't notice the poor pressure management as what is happening, but they notice the urinary leaking, the heaviness feeling, the low back pain, the tightness in the hips, the feeling of a weak core.
Just because those are the symptoms that are felt, it doesn't automatically mean there is a pelvic floor weakness or damage.
Why the Pelvic Floor Gets Blamed
I don't blame anyone for thinking that their pelvic floor is the problem. Especially in a postpartum population, where the pelvic floor obviously had some changes. It's where the symptoms are felt and can sometimes be the most embarrassing functionally with respect to the symptoms. It's easy to think, “I leak, that means I’m weak, I must get it stronger”. But this is where sometimes the limitation of looking at the pelvic floor by itself can really get people stuck. They get the things they think are “weak”, stronger and still have the same problem.
This is the limitation at only looking at the pelvic floor in that area of the body, and not looking at how the pelvic floor is working as part of a system.
Outside of an anatomy context, it's like this: If you had a heatwave going on, and a transformer blows, it's easy to say, “oh that transformer was a problem”. But the reality is, the heat wave is the problem and overloaded the system, and the transformer was just the weak point in the system
Patterns of Poor Pressure Management
There can be many reasons that poor pressure management happens in the body. Sometimes there can be breath holding when performing a task, impacting that pressure on the pelvic floor. Other times it can be a change in pelvic/rib cage stacking position. Even not taking deep enough breaths, not allowing the diaphragm its full length, impacts the pelvic floor's ability to fully lengthen, limiting its ability to sustain a load. Often in a postpartum population, that pelvis and ribcage are accommodating a growing belly, but the body never picks up correctly to go back to where it once was when that space is empty again. And still other times, there can be weakness in other areas of the body, like the abdominal muscles, that isn't supporting the front as much as it could, and therefore, the body then relies on the pelvic floor to carry more than it is prepared for, or just isn't coordinated well with those muscles.
All these different strategies the body is doing impacts where pressure gets re-disrupted to, and can impact the pelvic floor management of the pressure and whether you can remain with or without symptoms.
Pelvic Floor is a part of a team
When speaking about pelvic floor function and purpose in the body, it is important to understand that it is never working in an isolated context. The pelvic floor works in coordination with the diaphragm and transverse abdominal muscles, helping manage the intra-abdominal pressure. This pressure is a necessary thing in our bodies, and is vital for our internal organs to be able to do their job. Our body is going to prioritize this internal movement, and need to manage the pressure. When that pressure is optimal we generally feel like we're moving well, and when it's not, our organs are still getting what they need, but things like leakage and pain may be present.
Treatment
What this means on a treatment side, is shifting the mindset away from “I just need to strengthen my pelvic floor” to understanding our body’s specific pressure strategy, restoring coordination of muscles working together, and integrating breathing with movement.
Some examples of this can be:
When you lift something heavy, exhaling during effort
Learning how to stack ribs over pelvis in sitting, quad, and standing positions
Weight training with good breathing technique and coordination
Gradually building confidence in different positions and adding in more dynamic activities challenging positions when managing pressure
While the impact of leaking and heaviness can be very limiting in a postpartum population, understanding how the system works all together can be very empowering: no matter the severity of the symptoms. Avoiding the activities is not the solution, but rather understanding how to manage the pressure makes approaching the activities can be what allows the ability for someone to return to a previous activity or movement without fear.
The amazing thing about our bodies is the ability to adapt to changes. Most of the time those changes and compensations serve to keep us functional. Even when those changes are not serving us, our bodies still have the amazing capabilities to be taught even different strategies. Sometimes we can figure them out on our own, but other times, we need that support to figure it out.
If you are experiencing symptoms, it doesn't mean something is “wrong” with your pelvic floor, but rather, your body is just indicating it needs a different strategy. And with the right approach, that is something that can change.
REFERENCES:
Bø, K. (2004). Pelvic floor muscle training is effective in treatment of female stress urinary incontinence, but how does it work? International Urogynecology Journal, 15(2), 76–84.
Bø, K., & Stien, R. (1994). Needle EMG registration of pelvic floor muscle activity in nulliparous healthy females during voluntary contractions and Valsalva maneuver. Neurourology and Urodynamics, 13(1), 69–77.
Cholewicki, J., & VanVliet, J. J. (2002). Relative contribution of trunk muscles to the stability of the lumbar spine during isometric exertions. Clinical Biomechanics, 17(2), 99–105.
Hodges, P. W., Eriksson, A. E., Shirley, D., & Gandevia, S. C. (2005). Intra-abdominal pressure increases stiffness of the lumbar spine. Journal of Biomechanics, 38(9), 1873–1880.
Hodges, P. W., & Gandevia, S. C. (2000). Activation of the human diaphragm during a repetitive postural task. The Journal of Physiology, 522(1), 165–175.
Kolar, P., Sulc, J., Kyncl, M., Sanda, J., Neuwirth, J., Bokarius, A., … Lewit, K. (2012). Stabilizing function of the diaphragm: Dynamic MRI and synchronized spirometric assessment. Journal of Applied Physiology, 109(4), 1064–1071.
Neumann, P., & Gill, V. (2002). Pelvic floor and abdominal muscle interaction: EMG activity and intra-abdominal pressure. International Urogynecology Journal, 13(2), 125–132.
Sapsford, R., Hodges, P., Richardson, C., Cooper, D., Markwell, S., & Jull, G. (2001). Co-activation of the abdominal and pelvic floor muscles during voluntary exercises. Neurourology and Urodynamics, 20(1), 31–42.
Smith, M. D., Russell, A., & Hodges, P. W. (2007). The relationship between incontinence, breathing disorders, gastrointestinal symptoms, and back pain in women: A longitudinal cohort study. Clinical Biomechanics, 22(4), 401–408.
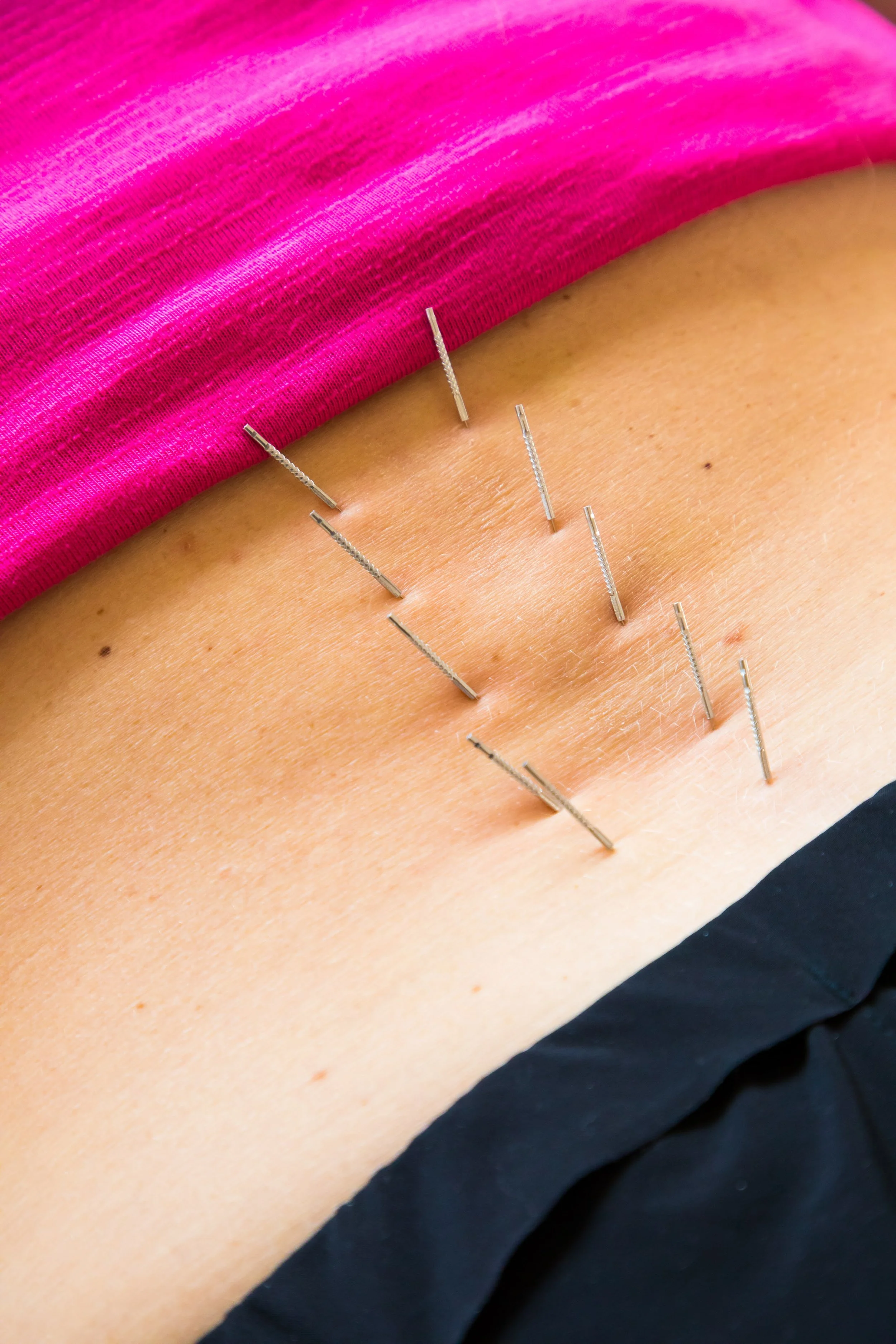
Dry Needling your back for pain, isn’t just about your back
A person walks into a clinic, after they strained their back last week with ongoing pain. They have tried all the tricks on their own to relieve it: heat, ice, stretching, pain patches; but nothing makes it better. They are offered dry needling, and they start to have some relief, and they start to feel better.
On the surface, the assumption is the needles went into the tight muscles, the muscles relaxed, and the pain went away. But in actuality it's much more interesting than that. Dry needling is not just about a localized treatment to the back. Those needles going into the back are impacting that area, but they are also influencing the entire nervous system.
Once you understand why dry needling works on the local level, you then can also understand why that matters in the long term.
Pain is complex:
Most people just understand the local level influence:
Needle goes into a tight muscle → the muscle relaxes → pain goes away
While this does occur at the specific sight of entry, this is an incomplete understanding of the process. Pain is not just a tissue or biological problem. This is especially true for pain that has been persistent or recurring pain that just doesn’t fully go away.
Pain is an output of the brain/nervous system, and not an input from the body. Our pain is not just an interpretation of what was hurt, but also layers with psychological and sociological aspects surrounding that experience on top of the biological (biopsychosocial). That’s why it’s often referred to as multifactorial experience and only treating the biological or tissue side sometimes doesn't help.
Nervous System Basics:
Our Nervous system is made up of 2 different parts:
Central nervous system (CNS) which is made up of our brain and spinal cord; our body's primary control center for processing information, coordinating behavior, and maintaining homeostasis (balance in our body)
Peripheral nervous system (PNS) which is made up of our nerves outside the brain and spinal cord, acting as a communication network between the central nervous system (CNS) and the body's muscles, organs, and skin.
Our PNS is made of then 2 parts the Somatic Nervous System (SNS) (the side we control our muscles and movement, think voluntary control) and Autonomic Nervous System (ANS) (the side that is involuntary control: Sympathetic and Parasympathetic)
The sympatric and parasympathetics of the ANS require homeostasis or balance for us to be functionally well. We often break this down into parts of a “Fight or Flight” as the sympatheics and “Rest, Relax and Recover" as our parasympathetics. When these two sides are not in a balance with each other, that can “throw off” the ANS and impact how our body perceives pain.
Things that can push you more into the sympathetic side such as poor sleep, high stress, workload balance, postpartum changes, and training load levels, can all impact how that ANS is functioning.
Any pain, and in this case, back pain can be directly influenced by what is going on in the ANS and how “on edge” the system is acting.
Back to the Back Pain:
If someone is in pain, or they strained their back, many times our body will go into a protection mode. The muscles surrounding the area of the perceived pain, tighten to guard the area and protect it. Over time, that area can then have increased sensitivity, meaning, it doesn't take as much influence of perceived injury to the area, to elicit the pain response. Then the brain starts to change how and what you are doing, to reduce the chance of it starting to hurt. We then all of a sudden can’t bend forward without feeling some type of pain.
When this cycle continues for longer periods of time without resolving, we then become more influenced by certain factors. While the back may have started out as the problem spot, it may not actually be the back that is the problem, but its responding to the environment around it.
Examples of this can be the way you are sitting at your desk, while you are stressed with a work deadline; the influence of postpartum mom, who is also now having to lift and carry 10lbs throughout her day; starting a new workout routine and sleeping poorly.
So the treatment for treating the pain is not just about the muscles in the area of the perceived pain, but also treating the whole nervous system.
Dry needling for pain
Dry needling does work at a local level. We know this from studies that show when inserting the needle into a trigger point, you can get a local twitch response, we get increased blood flow to the area, and muscle tone can be reduced in that area, which can be contributing to the local pain. But this is only a part of the effects of the dry needles.
Dry needling also impacts the Autonomic system, allowing for changes in the processing of the pain. The effects of the dry needles on the parasympathetic side of the nervous system causes the body to shift out of that “fight or flight” mode, into more of the calming/relaxing side. This is why people will sometimes report feeling calm, relaxed or sleepy post dry needling sessions. When this is happening, the body is shifting out of that protective mode, contributing to less guarding and less pain sensation. When our body is not feeling guarded or in pain, we have the ability to actually move better. Moving better is actually a key component to getting out of pain, because you are teaching the body that it is safe to move, and the response to stop the movement is diminished. When our bodies perceive the feeling of safety with movements, the alarm bells of pain are quieter.
This is ultimately what leads to feeling less pain post dry needling, and actually feeling better.
Why Exercise Still Matters Most
While quieting the pain sensation is an important part of moving better, dry needling alone is usually not enough. Dry needling isn’t about “fixing” your back, it’s a tool to help you move with less discomfort so you can get back to the strength and mobility work that actually drives long-term change in our bodies, allowing your body to adapt itself. Dry needling needs to be paired with strength training, mobility work, and load management in order for the body to truly recover function. Dry needling with exercise is how you start to feel better, but then also start to move better so the pain does not come back. Exercise also is acting on the nervous system, retracing the brain and nervous system that it is safe.
So that person that comes in feeling better after 2-3 sessions isn’t typically done in their rehab journey. The good thing is the pain is usually no longer the barrier to actually moving. The movement and exercise is what we know actually will help them stay better and help keep their body more resilient in the long term.
It’s Bigger Than the Needle
Dry needling is so much more than releasing a tight muscle. It's impacting an entire nervous system that is influencing that muscle. When we have pain, it does not mean our bodies are broken, it just means our bodies are adaptable to the influences on it. When we can change how the system responds, we can change how our bodies can move.
And because our pain is multifactorial, treating pain just at a local level will help, but doesn’t change the pain in the long term.
References:
Bialosky JE, Kearns WD, George SZ.
Dry Needling and Acupuncture for Musculoskeletal Pain: Mechanisms and Clinical Implications.
Physical Therapy Reviews. 2010;15(4):263–267.
Dommerholt J.
Dry Needling — Peripheral and Central Considerations.
Journal of Manual & Manipulative Therapy. 2011;19(4):223–227.
Langevin HM, Churchill DL, Cipolla MJ.
Mechanical Signaling Through Connective Tissue: A Mechanism for the Therapeutic Effect of Acupuncture.
FASEB Journal. 2001;15(12):2275–2282.
Dunning J, Butts R, Mourad F, et al.
Dry Needling: A Literature Review with Implications for Clinical Practice Guidelines.
Physical Therapy Reviews. 2014;19(4):252–265.
Fernández-de-Las-Peñas C, Nijs J.
Trigger Point Dry Needling for the Treatment of Myofascial Pain Syndrome: Current Perspectives Within a Pain Neuroscience Paradigm.
Journal of Pain Research. 2019;12:1899–1911
Boyles R, Fowler R, Ramsey D, Burrows E.
Effectiveness of Trigger Point Dry Needling for Multiple Body Regions: A Systematic Review.
Journal of Manual & Manipulative Therapy. 2015;23(5):276–293.
Cagnie B, Dewitte V, Barbe T, et al.
Physiologic Effects of Dry Needling.
Current Pain and Headache Reports. 2013;17(8):348.
Kietrys DM, Palombaro KM, Azzaretto E, et al.
Effectiveness of Dry Needling for Upper-Quarter Myofascial Pain: A Systematic Review and Meta-analysis.
Journal of Orthopaedic & Sports Physical Therapy. 2013;43(9):620–634.
Shah JP, Thaker N, Heimur J, et al.
Myofascial Trigger Points Then and Now: A Historical and Scientific Perspective.
PM&R. 2015;7(7):746–761.
Perreault T, Fernández-de-Las-Peñas C, Plaza-Manzano G, et al.
Dry Needling in Physical Therapy Treatment of Chronic Pain: Systematic Review.
Journal of Clinical Medicine. 2024;13(4):1123.